Medicine Elog
Cheif complaints: A 46 years old female who is a agricultural labour came with c/o SOB exertion since one week c/o abdominal distension since last week patient was apparently asymptomatic one year back and then devoloped dyspepsia for which she started using tablets on and off and was fine after taking tablets then she devolped SOB since one week which was not associated with chest pain and palpitations
HOPI: Pedal edema , cough . patient noticed a swelling in epigastric region during exertion and she also devolped abdominal distension since one week no h/o of cough ,cold and fever 
History of past illness :
No h/o chest pain,palpitations and PND
No h/o headache
No h/o burning micturition
N/K/C/O HTN , DM ,TB , epilepsy ,asthma
Personal history : normal apetite
Bowels : Regular
Micturition : normal
Habits : Alcohol-No
Tobacco Snuffs and chewables -No
Family history:
DM : No
HTN :No
TB : No
Asthama : No
Any personal or hereditary diseases:No
Physical examination:
Pallor : No
 |
| No pallor |
Icterus :No
Cyanosis :No
Oedema of feet : No
Temp : 99 degree F
Pulse ;86/min
Bp : 120/80 mm hg
Clubbing of fingers
Systematic examination:
Abdomen:
Shape of abdomen : Distended
Tenderness : yes
Palpable mass : yes in epigastric region
Liver : not palpable
Spleen : not palpable
Respiratory system:
No disponea no wheeze and position of trachea is central nd breath sounds are vesicular
CVS : No thrills and no cardiac murmurs
CNS : level of consciousness is alert and speech is normal
Investigation : Hemogram, CUE HbsAg rapid,blood
Sugar random, serum electrolytes ultra sounds at abdomen were taken
Diagnosis: Acid peptic disease with denova detected type 2 DM with epigastric hernia further treatment proceeded with surgery
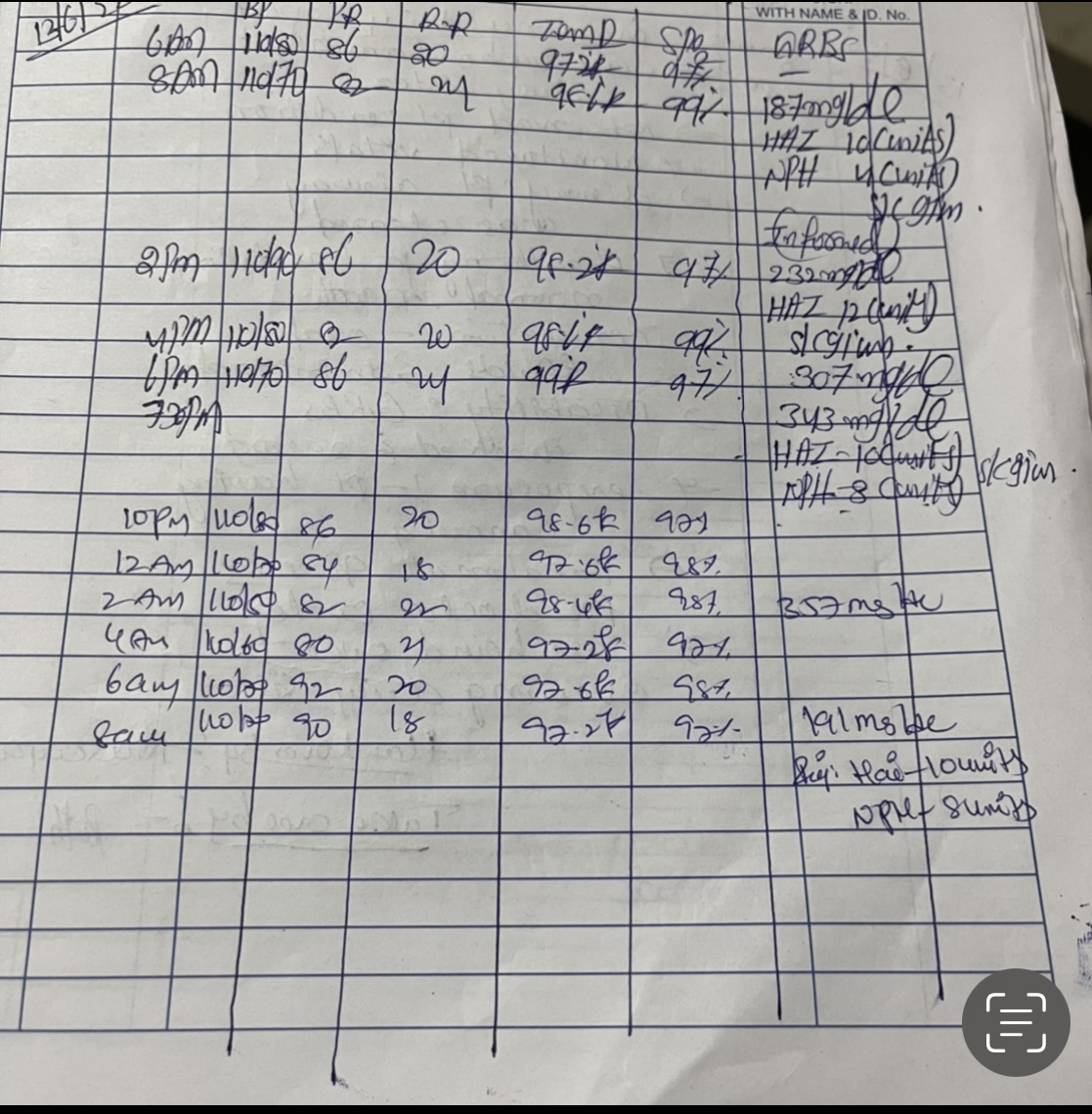
Treatment:
Inj:HAI with regular interval
Inj:NPH with regular interval
Inj : PAN 40 mg
Inj : opineuron amp


{kind=link}
 Q1 what is the anatomical location of the patients problem ?
Q1 what is the anatomical location of the patients problem ?
What is an epigastric hernia?
An epigastric hernia is a lump in the midline between your belly button and sternum (breastbone) which can cause pain.
Your abdominal cavity contains your intestines and other structures. These are protected by your abdominal wall, which is made up of four layers.
In an epigastric hernia, fat pushes out through a weakness in the wall of your abdomen between your belly button and sternum and forms a lump. The most common symptom is pain caused by the fat being pinched by your abdominal wall.
Peptic ulcer disease is characterized by discontinuation in the inner lining of the gastrointestinal (GI) tract because of gastric acid secretion or pepsin. It extends into the muscularis propria layer of the gastric epithelium. It usually occurs in the stomach and proximal duodenum. It may involve the lower esophagus, distal duodenum, or jejunum. This activity reviews the cause, pathophysiology, and presentation of peptic ulcer disease and highlights the role of the interprofessional team in its management.
Q2.why is the patient having this problem?
An epigastric hernia is usually present from birth. It forms as the result of a weakness in the abdominal wall muscles or incomplete closure of abdominal tissue during development.
Some factors that may cause or exacerbate epigastric hernias include:
- obesity
- pregnancy
- coughing fits
- heavy lifting
- physical labor
Causes of acid peptic disease include:
- Helicobacter pylori: H.pylori is responsible for around 60%-90% of all gastric and duodenal ulcers.
- NSAIDs: Prostaglandins protect the mucus lining of the stomach. Non steroidal anti-inflammatory drugs (NSAIDs) such as aspirin, diclofenac and naproxen prevent the production of these prostaglandins by blocking cyclo-oxygenase enzyme leading to ulceration and bleeding.
- Smoking, alcohol and tobacco: Cigarettes, alcohol and tobacco cause an instant and intense acid production which acts as though gasoline is poured over a raging fire!
- Blood group O: People with blood group "O" are reported to have higher risks for the development of stomach ulcers as there is an increased formation of antibodies against the Helicobacter bacteria, which causes an inflammatory reaction and ulceration.
- Heredity: Patients suffering from peptic ulcer diseases usually have a family history of the disease, particularly the development of duodenal ulcer which may occur below the age of 20.
- Steroids/Other medicines: Drugs like corticosteroids, anticoagulants like warfarin (Coumadin), niacin, some chemotherapy drugs, and spironolactone can aggravate or cause ulcers.
- Diet: Low fiber diet, caffeinated drinks and fatty foods are linked to peptic ulcer
- 3. What are we doing about it ?
- Pharmacological: Inj : hai
- Inj : nap
- Inj:opineuron
Comments
Post a Comment